1.1 Does the first domain need to be successful before a subsequent domain is started?
Funding constraints are preventing the start of other domains. If we secure additional funding or medications, other domains will start. It is not dependent on the success of the first domain.
1.2 Does a domain need to be complete before a subsequent domain is started?
No, participants can be enrolled into a new domain at any time.
1.3 Can a patient participate in two domains at the same time?
Yes, a patient can participant in more than one domain at the same time.
1.4 How can new staff members at sites be trained on trial procedures?
New staff can review SIV slides and study documentation. Regional Coordinating Centres can provide training, including refresher training, upon request.
2.1 Can patients be recruited if they do not tolerate ACEi/ARBs?
Yes, patients can be recruited as long as all standard of care therapies appropriate to their region have been offered to them.
2.2 Is current kidney transplant an exclusion criterion for the study?
While current kidney transplant is not an exclusion criterion for the platform, it is for the MRA domain. The exclusion criteria for the platform and individual domains are kept separate in the study.
2.3 Can patients receiving immunosuppressive therapy be recruited into the trial?
Yes, patients receiving immunosuppressive therapy can be recruited.
2.4 Can patients with high eGFR, for example eGFR > 85 ml/min/1.73m², be recruited into the trial?
Yes, they can be recruited. There is no upper cut off limit for eGFR.
2.5 Can the Screening visit and Randomisation visit be held on the same day?
The Screening visit and Randomisation visit can occur on same day provided that blood test and urinalysis test results are from different days. This requires the use of prior, standard of care pathology results (dated up to -31 days before randomisation) for the Screening visit. Blood and urinalysis tests for the Randomisation visit must occur on same day as randomisation. This is important as baseline eGFR and uACR is the average of 2 values from the screening and randomisation visits.
3.1 Are blood tests and urinalysis performed at local labs?
All pathology is performed at local labs and there are no central labs. Standard of care tests can be used if they fall within visit windows. For the randomisation visit, pathology will likely need to be performed for the trial as it is unlikely a test result is available from routine clinical care.
3.2 Can a patient remain in the trial if standard of care (SOC) treatment changes; for example, if the patient stops ACEi/ARB?
Yes, the patient can remain in the trial even if their SOC treatment changes.
3.3 Can a patient remain in the trial if standard of care (SOC) treatment guidelines change; for example, if a new treatment is considered SOC?
Yes, the patient can remain in the trial even if SOC changes. We will collect data on what treatments a patient is receiving at all visits.
3.4 Should the study intervention be stopped if patient commences on dialysis or has a kidney transplant?
Yes, the study intervention should be stopped if a patient starts on dialysis or has a kidney transplant. This is a study end point.
4.1 How will passive follow up be conducted?
We plan to follow patients every 5 years using medical records. Sites will be asked to check patient medical records to assess survival (dead or alive) and kidney (receiving dialysis or transplant) status. Data linkage may replace review of medical records in jurisdictions where it is available.
4.2 How are unknown dates entered into the eCRF?
If the exact day is not known, enter ’15’ for day. If the month is not known, enter ‘June’.
5.1 What is the primary outcome for CAPTIVATE and how was this selected?
The primary outcome for CAPTIVATE is chronic estimated glomerular filtration rate (eGFR) slope (mL/min/1.73m2/year) estimated from all available “on-treatment” eGFR values from week 4 to week 104.
Large trial data have demonstrated that eGFR slope is a valid surrogate endpoint in phase 3 randomised controlled trials in chronic kidney disease (CKD) (Levey et al. AJKD 2020). This allows for smaller sample sizes and shorter trial durations compared to traditional “hard” kidney outcomes such as kidney failure. Several therapeutic agents that may potentially improve kidney outcomes in CKD and will be tested in CAPTIVATE produce initial haemodynamic effects, resulting in an acute “dip” in eGFR which typically occurs within the first 4 weeks. To mitigate the risks of type 1 errors, one approach is to utilise chronic eGFR slope, i.e. exclude the values during the acute period. Another method is to use eGFR values from randomisation to the end of a washout period to evaluate total “off-treatment” slope. Extensive expert discussions, statistical analyses, and trial simulations have been conducted to reach this final decision to use chronic eGFR slope as the CAPTIVATE primary outcome and the reasons are as follows:
- The use of chronic eGFR slope ensures consistency between the primary outcome and interim analyses, as off-treatment washout values are not available for those undergoing interim analyses.
- Excluding values during the acute eGFR dip will reduce statistical complexities and risk for error as additional domains are added and combination therapies are studied.
- The required sample size for assessment chronic eGFR slope is smaller than that for total eGFR slope.
- Importantly, chronic eGFR slope has been demonstrated to be a stronger predictor of kidney outcomes.
- For additional sensitivity analyses, we have included total eGFR slope measured from week 0 (randomisation) to week 108 (end of washout) as a secondary outcome.
Reference: Levey AS, Gansevoort RT, Coresh J, Inker LA, Heerspink HL, … Levin A, Perkovic V, Zhang L, Willis K. Change in Albuminuria and GFR as End Points for Clinical Trials in Early Stages of CKD: A Scientific Workshop Sponsored by the National Kidney Foundation in Collaboration With the US Food and Drug Administration and European Medicines Agency. Am J Kidney Dis. 2020 Jan;75(1):84-104. doi: 10.1053/j.ajkd.2019.06.009.
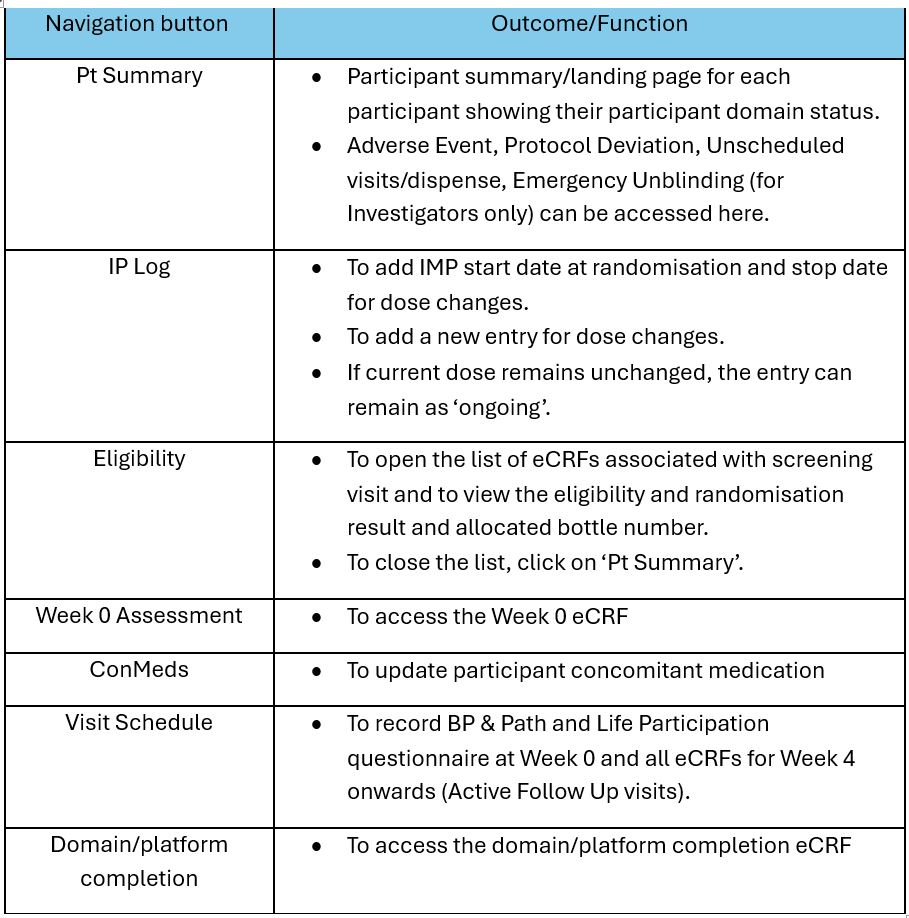
7.1 How can a site access specific study visit eCRFs and logs in the database?
The table below is a guide on how to access study visit eCRFs and logs from the Participant Summary Page:
7.2 How can a site access the ‘Consent & Eligibility’ eCRF for participant that was previously pre-screened?
To access the ‘Consent & Eligibility’ eCRF for participant that was previously pre-screened, go to the participant’s pre-screening record and click on ‘Continue’. The ‘Start Eligibility’ button will appear if the participant is deemed eligible at pre-screening.
7.3 How can a site enter unknown dates in the eCRF?
- *Unknown Day*: If the exact *day* of the month is not known, enter *’15‘* for the day.
- **Unknown Month*: If the exact *month* is not known, enter *’June‘* for the month.
By following this guidance, the data will maintain consistency across the system while accounting for any uncertainties regarding dates.
7.4 How can study staff opt-in or opt-out to receive automated email notifications?
To opt-in or opt-out to receive automated email notifications, go to ‘My Details’ under your account and click on ‘Emails’. Select ‘√’ to receive email alerts or ‘X’ to opt-out.